This edited talk, presented as the 2025 Melissa Harte Memorial Lecture (4th Feb 2025), explores the contribution that person-centred thinking and practice can make to social justice; the limitations of this approach; and the potential for powerful, original, and exciting synergies between person-centred and social justice perspectives. The work, here, overlaps with a range of person-centred writings: such as Gillian Proctor on power, Colin Lago and colleagues on difference and diversity, and Gay Barfield on peace work. However, drawing on my recent book Psychology at the Heart of Social Change: Developing a Progressive Vision for Society (BUP, 2023), I hope that it also opens up new perspectives and possibilities. The video recording of the original talk is available here.
To start with some personal background: the question of social justice has, for me, been of critical importance throughout my life. I came from a progressive family: my parents were members of the Communist party. But that was the Highgate Communist party, and if you know where Highgate is in North London, you’ll know it’s a fairly affluent area. So there was some irony in having Communist party meetings in these very plush living rooms. Both of my parents’ families were working class emigrants from Eastern Europe: Jewish immigrants who’d experienced through their families a lot of what we call now intergenerational trauma and oppression. For my dad, who became very involved in the Communist party in the 1930s, social justice was a driving force for him in his life. And for me and my sisters, he really inculcated the sense that a meaningful life was one of trying to make a positive difference to the world. That’s a striving that I’ve carried through in my life, up to my latest book, Psychology at the Heart of Social Change, which tries to show how person centred psychological ideas can contribute to a broader and a wider understanding of what social change possibilities might be in a better world; and my involvement with the Therapy and Social Change (TaSC) Network.
Social justice is the ‘fair and equitable distribution of resources, opportunities, and privileges within a society ensuring that all individuals, regardless of race, gender, socioeconomic status, or other characteristics, have equal access to rights and opportunities’ (ChatGPT—my new best friend!). Social justice is fundamentally about fairness, equity: about people having equal opportunities.
If you go back into the history of the person-centred approach, it did not evolve as a social justice approach. It evolved, with Rogers, as a clinical approach, and as a way of helping families and young people and adults to find greater well-being and to thrive. However, I think it really has a concept of fairness at its core. In the person censored approach, right at the heart of the approach, is the idea that the therapist isn’t somebody who is ‘better’ than the client, but someone who trusts the client: who sees them as an agentic, responsible human being—essentially, somebody who is like us. That is, in many ways, the unique quality of the person-centred approach. It’s an ethic—maybe not explicitly, but implicitly. And, I think that is what draws so many people to the person-centred approach: because, like me, when they read Rogers, they love this idea that the therapist—rather than being an expert in the client’s life, rather than being the person who comes in and says, ‘Right, I know what you need to do; you do this, this, and this, and this, and that will sort you out’—is actually someone who listens to the client. That is, someone who listens carefully, trusts, and appreciates the wisdom of the client. And that’s about equality. There’s a principle there of, ‘I’m not better than you’, but ‘You and I have a shared humanity that defines who we are and defines what the person-centred approach is.’
What I want to suggest in this talk is that the person-centred approach has a real contribution to make to social justice thinking and practice. But, at the same time, I want to suggest that there are ways in which the person-centred approach is limited, and that if we want to develop a really strongly social justice-based perspective, then there’s more that we need to take into the person-centred approach. This is a synergy between person-centred and social justice: to create something that could be so special and so powerful and so badly needed in the world today.
The Contribution of the Person-Centred Approach to Social Justice
So why might the person-centred approach, the thinking of Carl Rogers and the work since him, have so much to contribute to social justice? What the person- centred approach introduces is this idea, as discussed earlier, of psychological equality. And it’s not just seeing the other as equal in terms of how they might be or how they could be, but in their very core: in the very essence of their being. It’s an acceptance in their genuine, authentic being.
That really deep, powerful acceptance is something that many ‘social justice’, ‘progressive’ perspectives today don’t always have. They have a notion of equality. They have a notion of fairness, but often it’s a fairness at the social and at the economic level only. What’s missing is that fairness, that understanding, that depth of equality as one human being to another. ‘Social justice’ perspectives—for instance, Labour perspectives and Green perspectives in the UK—can sometimes really move into a ‘politics of blame’: where those who disagree with us are seen as bad or malevolent, they become demonized. If you look, for instance, at how left-wing MPs can talk to their opponents in political debates, or Prime Minister’s Question Time. Or if you look at election manifestos, the ways that, for instance, Labour talk about the Greens or the Greens talk about Labour. Even somebody who has a slightly different view on something—rather than being seen as another fellow human being who is doing their best to articulate and put forward a viewpoint, is often demonised, is blamed, is criticized, is seen as fallible and even malevolent. And although, for me, it’s really understandable that we can adopt those perspectives (I know I can do it myself), I think it betrays the very principles of social justice; which is a really deep, abiding valuing of everyone and their due.
So, as I state in my recent book, to deepen and advance progressive thinking and practice, we need to move from a politics of blame to a politics of understanding, and that’s one in which even our political opponents are engaged with in empathic, valuing, and caring ways. And that’s where I think the person-centred approach, with its unconditional positive regard, empathy, and congruence, has so much to offer to social justice perspectives and practices. Michael Lerner argues for something similar when he talks about a stance of revolutionary love. Lerner talks about this as a ‘socialism of the heart’, and he describes it as the love of life in all beings embracing this world with all its complexities, heartaches, and joy. It’s an approach that is caring towards everyone on the planet, even those whose behaviour we hope will change, and towards the earth in all its magnificent diversity as well.
This stance of radically accepting the other, whoever the other is, is, I know, massively controversial for progressives. Does it mean accepting people like Trump? Does it mean saying, ‘Wow! He’s such a nice guy’, we can’t criticize him. That certainly isn’t what I’m suggesting. Rather, that commitment to seeing the other as psychologically equal can run alongside a fundamental commitment to economic, political, and social equality—and being willing to challenge those who undermine it. But, despite such challenges, it is a willingness to view the other, every other, as a human being like ourselves, with needs, wants, and experiences that are, in the words of R. D. Laing, ‘intelligible’ and meaningful. In the terms of Rogers, it’s about seeing all others as striving to maintain and enhance their being: that those needs and wants are legitimate from that person’s subjectivity. It’s an openness to putting ourselves in the shoes of the other, and to taking the other’s perceptions seriously, just as we want them to take ours. Bhasker Sunkara, author of The Socialist Manifesto, said that, at its core, to be a socialist is to assert the moral worth of every person, no matter who they are, where they’re from or what they did.
In other words, when we engage with others from the assumption that we’re right or good and they’re wrong or bad, we betray a core principle of social justice thinking: that all people are of equal worth. And the person-centred approach gives us a way of moving beyond that politics of blame to one which, while still able to critique certain behaviours and say that certain behaviours are damaging, can hold that worth of people. Karl Marx’s favourite maxim was, ‘Nothing human is alien to me’, which is actually what many people say is the defining quality of humanism’. And that needs to apply from us to them, from Left to Right, as well as from them to us. That principle of psychological equality means moving beyond the demonization of the other. It means moving towards a politics of holding and prizing the other; beyond seeing our political enemies as inherently evil, manipulative, deceitful; beyond a James Bond-type world of ‘baddies’ and ‘goodies’. It doesn’t mean that we can’t oppose people who act in oppressive ways, it doesn’t mean we can’t challenge them, it doesn’t mean we can’t even use force to stop them hurting others. But in all this it means not turning the other into a monster. It means holding on to their humanity with a care, compassion, and the egalitarian spirit that is at the heart of a social justice vision.
This belief in the goodness and capability of human beings is rooted in my own personal journey. When I was a child, and I used to go to school and tell my schoolmates that I was a Communist, the first thing people would say to my sister and myself is, ‘Do you believe in money?’ and we’d say ‘no’. And people would say, ‘Well, that’s not going to work because everybody would just go to the shop and take whatever they want.’ I remember imagining people going to the local sweet shop and taking all the packets of sweets off the counter and stripping the shelves bare. But my sister and I used to have a pre-prepared answer: ‘Well, actually, people won’t do that. People are inherently good. And it’s money, society, that makes people bad.’ That conception of people as basically good is really still with me—albeit, I hope, in more sophisticated and nuanced form. But it comes from that person-centred commitment to psychological equality: a commitment that I still believe needs to be at the heart of a progressive/socialist/green outlook. Because it just seems to me deeply arrogant, patronizing, and hierarchical to think ‘I’m right’, ‘I’ve got the answers’, ‘Other people are less moral, less capable, less right than I am.’ If I see the world in that way. If I see myself as right and the other is wrong, then how am I different from any other perspective that holds, ‘I’m right. I’ve got the answers. I’m better than you’?
A second reason why I believe in the essential ‘goodness’ of others is that, if others aren’t actualizing, if they don’t have that potentiality or aren’t able to do that, then where does that lead? Does that mean that a socially-just society would need to be enforced at the endpoint of a gun: that we would need laws and regulations and force to keep people within an equitable way of being? To have a positive, thriving, socially just society, we need a vision that people can cooperate, people can work together: that people can do the best, given the possibilities and given the resources to do so.
Also, if we want to create a better society, we need to understand what people really need and want: what really motivates people. If we blame people, if we see people as demonic and bad and malevolent, we miss a deeper understanding of others. Developing a better society starts with asking what it is that people need and want: what would better look like, more of what? And I think, as therapists, that’s something we’re doing all the time: understanding people in terms of their deepest needs and wants. That is, understanding their strivings to grow; understanding people in terms of that desire for relational depth; striving, as in Rogers’s theory, for self-esteem; striving for freedom; striving for meaning. These are all things that, by sitting alongside people, empathising with people, we come to understand. What we learn as therapists is that it’s very rare that you sit with somebody—whether you work in person-centred ways or otherwise—and think, ‘My God, this is just a really bad person.’ What you see, rather, is that sometimes people do damaging things, but it nearly always comes about because they’re striving for things which, ultimately, aren’t ‘bad’: like a desire for relationality or self-worth.
So I think a person-centred attitude would allow those interested in social justice, those on the Left, those working towards a more equitable society, to understand more about what it is that people deeply want. There’s some really interesting developments at the moment around ‘wellbeing economics’. This has become very influential in places like New Zealand and in some of Scandinavia where governments, rather than thinking, ‘How do we maximize GDP?’ are thinking, ‘How do we maximize wellbeing?’ And there’s some really interesting kinds of calculations used to work out wellbeing. But it’s all got to start from this question, ‘What is it that people want? Where is it that people want to go to?’ The person-centred approach has got some great answers for that. And, in our experience as therapists, we don’t just see what people want, we experience it. I know, for myself, that when I’m sitting with clients there’s a powerful sense of another person striving towards growth and development: striving, not just for themselves, but also for others. I don’t think I’ve ever worked with a client who’s just thought about themselves. I’ve worked with clients who often struggle between the need for self and need for others, but there’s always some element of the other there in the self. And it’s something that I experience. It’s something that we deeply know, because we’ve been alongside it. Of course, as psychotherapists and person-centred therapists, we don’t have all the answers, but I do think we have something very important in terms of that lived, experiential sense of where people are striving to go to, and what people are like at that very directional core.
Of course, in Rogers’s lifetime this commitment to meeting others through a lens of psychological equality was applied and extended to thinking about politics and thinking about social justice. Rogers says, as quoted by Gay Barfield, ‘I find for myself, I’m most satisfied politically when every person is helped to become aware of his or her own power and strength.’ Rogers, in his work, was deeply political and deeply committed through his ideas and through the person-centred approach to making a change at a wider level. That was probably most manifest in Rogers’s peacework. Maureen O’Hara writes:
In his last years Rogers worked in over 20 countries, including South Africa, where he facilitated encounters between blacks and whites, Latin America, where North encountered South Europe, where Eastern bloc Marxists met Western humanists. Ireland, where Protestants met Catholics in Rust Austria, where he brought together diplomats, politicians, and peace activists from Nicaragua, the United States, and other Central American and European countries, to consider the violence then raging in Central America. And to the former Soviet Union, where participants met each other in new and more open ways.
Rogers felt that the person-centred approach had a real contribution to make at that wider political level in terms of psychological equality, in terms of a vision of people as being able to talk and listen and work together. What you see in his Rogers’s peacework (see, for instance, his video The Steel Shutter of his work with Protestants and Catholics in Northern Ireland) is him really entering into the political sphere in such a unique, original, inspiring way. He brought ideas of the intrinsic value of every person from every community together, and believing that people can hold that value of each other, and that through that communication they can find solutions.
That’s something that has continued to have a contribution to make. And we see that in work continuing today, there’s work from the Peace Project people like Gay Barfield, who for many, many years been involved in that; Maria Kontarini; the work that John Wilson’s been doing with colleagues on Going Global; Maureen O’Hara in the United States on leadership and senator John Vasconcellos, who tried to bring Rogers’s ideas in to the American political system. And, there’s some really interesting work that Emma Tickle at the University of Nottingham and colleagues are doing on peace and the person-centred approach (see here). There’s also been some really impactful and far-reaching developments, that maybe wouldn’t be called strictly person-centred, but has been very much inspired by Rogers. For instance, nonviolent communication by Marshall Rosenberg: how we can communicate with others to avoid conflict by using ‘I-statements’ and owning our feelings rather than blaming the other. Parent Effectiveness Training from Thomas Gordon. Also, a lot of the social and emotional literacy training in schools: where they train young people, for instance, in developing empathy—a lot of this has roots in Rogers’s work.
So I think the person centred approach paves the way for a new kind of progressive politics; a politics that isn’t about blame, that isn’t about ‘I’m right and you’re wrong’. It’s a progressive, emotionally-literate politics that involves progressives taking the first step to genuinely act in non-defensive, cooperative ways: putting ourselves out there and taking the risk of trusting and being open to others. This is a politics which is about accepting and valuing the others, whatever their beliefs; trying to understand where people from different views come from, engaging in genuine dialogue. A politics that is about honesty, transparency, and congruence. Imagine politicians who could recognise, and be truthful, when they make mistakes and show vulnerability; who could be self-aware. And, also very importantly, politicians who can look after themselves and self-care. At TaSC, we’ve worked quite closely with a group called Compassion in Politics, and it’s very interesting to hear from them just how little self-care there often is in political environments.
Challenges to the Person-Centred Approach from a Social Justice Perspective
So, the person-centred approach has a unique place in social justice. But, despite that, we also have to recognise that, if we look at contemporary political movements—if I talk to my Gen Z kids about the things that are the forefront of their minds—things like the trans rights movement, Black Lives Matter, #MeToo, intersectionality, responses to the far right across Europe and America…The reality is that the person-centred approach hasn’t figured heavily at all. This is in terms of both action, and in terms of making sense of some of these issues. That’s not to say that people in the person-centred approach haven’t been involved individually. I know many people have got really involved and done really good work, but as a field we’ve yet to find a way of effectively responding and leading in these areas.
I think it’s also true to say that in the therapy field, in the US, for instance, the cutting edge of therapy is now work around multicultural counselling and social justice approaches—a ‘fourth’ or a ‘fifth’ force in therapy (see competences, for instance, here). And they would actively see themselves as something that has moved on, or even moved away from, a humanistic, person-centred approach. Not to say that they’d entirely reject humanistic or CBT or psychodynamic ideas and practices, but they clearly make a mark between social justice, multicultural approaches and approaches like person-centred therapy. Part of those social justice approaches is practices like broaching (where the therapist, deliberately and intentionally, introduces issues like race, as relevant to the client’s presenting concern) or advocacy (where the therapist is working alongside the client to help them with practical issues around, say, housing or welfare). These aren’t issues that have been theorized yet and worked into person-centred practice. Indeed, in multicultural and social justice practices, at those edge, they might even say that this is something opposed to more traditional non-directive ways of working.
So I think we need to ask ourselves, ‘What is it about the person-centred approach and person-centred thinking that maybe means that we haven’t been at the forefront of some of these developments?’
Much of it, I think, comes down to the individualism of person-centred thinking. It’s individualism that makes it difficult to integrate into the approach understandings and practices which take into account wider social factors, structures, and power dynamics: both in terms of what it means to be marginalized and be at the bottom of a power hierarchy; and also what it means to have power and what it means to be privileged. Emma Tickle was saying recently that perhaps the person-centred approach is very good at the individual level, and also in terms of universal human qualities. But where it perhaps isn’t so strong, is at that meso- level: in terms of people being members of classes, cultures, particular groups—and then the interfaces between those classes and cultures and the power dynamics between them.
Much of this is rooted in the individualistic assumptions that underlies the classical person-centred approach. The basic idea within Rogers is that we come into the world as an experiencing organism: a monad-like separate entity. And when we understand people in that way, we can certainly say that all human beings phenomenologically, experientially, are equal, and should have equal rights, and should have equal freedoms. And that’s very much there in liberal ideology. But what is more difficult to conceptualize when we think about people in that individual experiential, phenomenological way—as these phenomenological wholes—is how a priori, pre-existing structures, cultures, unfreedoms, imbalances in social and economic power resources really come in. If we start with this experiencing phenomenological organism, where is the place for these a priori structures?
In many ways we can compare it with a shift from Husserl’s phenomenology to Heidegger’s existential philosophy. Husserl’s focus tended to be on individual experiencing. Heidegger, who was really influential on so much contemporary thinking, emphasised more that human being is not a fixed, finite monad, but an openness, a receptivity to the world. We are embedded, or in Heidegger’s language, ‘thrown’ into a world. So we’re not a separate being in Heidegger’s thinking in quite the way we are in earlier Husserlian thinking. We are a ‘being-in-the-world’, we are influenced and embedded within the world.
Certainly, Rogers doesn’t say that we are not influenced by the world. But, for Rogers, it’s more that we come in as a whole being, and then the world infiltrates us and affects us and damages us in various ways. For Heidegger, by contrast, and for many people who then follow on—postmodernists, many feminists, people writing about sex and gender (like Judith Butler), multicultural thinking, posthumanistic thinking—it’s all founded around the idea that we are fundamentally embedded in the world. It’s interesting to compare the Rogerian and Heideggerian ideas of authenticity. For Rogers we come into the world as authentic, become inauthentic, and then therapy can help us return to an authentic state. But for Heidegger we are inherently inauthentic, because we are inherently thrown into a world that is beyond our making. We can find some kind of awareness of where we are in that. But we can never be truly separate in this ‘intersubjective’ model of the world. One of the popular ways of thinking about that embeddedness today is from Broffenbrenner. Many people will know the ecological systems model: the idea that you have the individual, and then you have the microsystem around them, then you have the community, then you have these wider levels. And the person is all these levels. There’s not a fixed individual who is separate from all these levels. But the person is fundamentally immersed in the world.
So, for instance, when we look at issues like race: from a liberal perspective, we might say white people and people of colour are equal. That would be fundamental. But if we start from an understanding of people as embedded in classes and in structures, in powers, in hierarchies, then it’s not just that people are phenomenologically equal. It’s also that they carry the weight of different structures that they are part of. Person-centred thinking certainly allows for an appreciation of marginalization: it has enormous ability to understand that experience of oppression. But what it lacks is that ability to understand the structural embeddedness of it. For instance, as a white person, I have a certain privilege, even though I might not feel privileged, but there is still a structural privilege that goes with that that doesn’t discount the fact that phenomenologically I may not feel privileged. There is this structural, economic, social privilege. In person-centred terms, we do take into account social factors, in the sense that people experience conditional positive regard, and certainly somebody could have conditions of worth as a female or as a male, and that could limit and oppress them. But we’re not just talking about conditions of worth here because we’re talking about economic, social, political, power-based realities that mean that there are dis-equities and imbalances that sit alongside the phenomenological experiencing.
This has real implications for practice. The basis of the ‘core conditions’ is the idea that, if we can create an open, unconditionally accepting space for someone, then it allows them to express their authentic truth and to grow and enhance themselves in whichever way is right for them. But it’s based, to a great extent, on the idea that people are on an equal playing field to begin with. If we start from a more embedded, contextualized understanding—that people are marginalized and disempowered by things like social injustices, racism, and poverty—then the work as a therapist isn’t just about providing a non-directional space, but to work to bring the person back up to a level of equity. That’s the approach of people who advocate for multicultural and social justice therapies and practices like broaching. Here, you can’t assume that people are starting on the equal level. There is a dis-equality which means that interventions need to support people to come back onto the equal level.
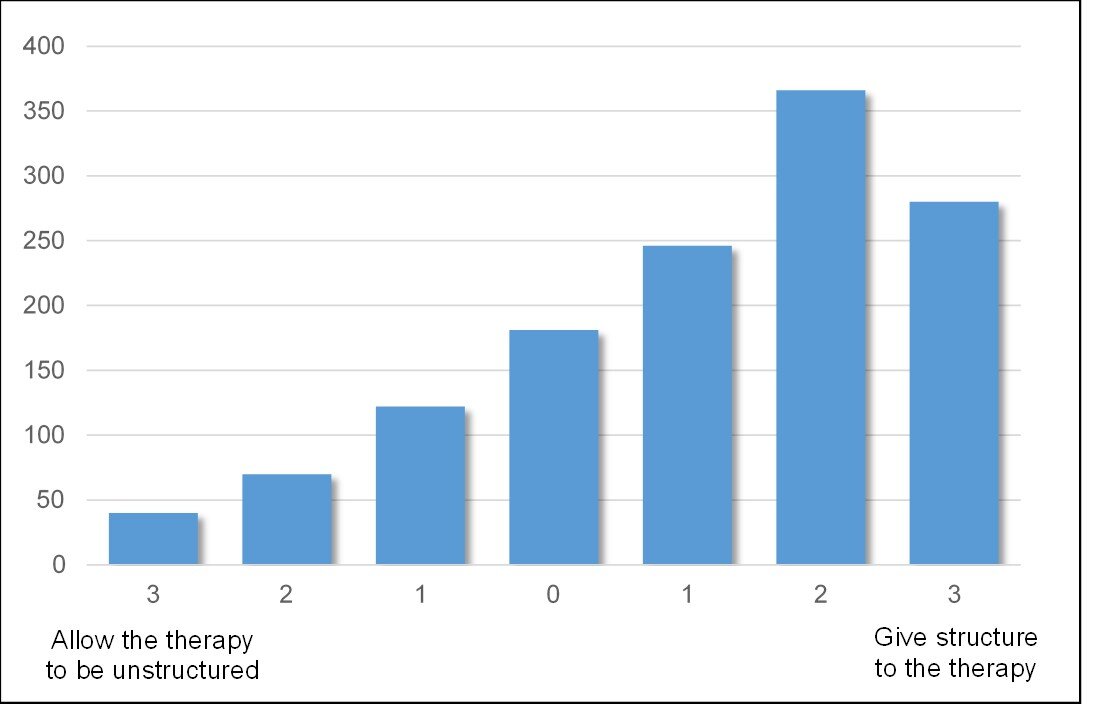
There’s kind of been similar discussions around what happens in groups. There was a really interesting paper written by Jo Freeman in the 1970s called ‘The Tyranny of Structurelessness’. She was talking about unstructured groups in the feminist movement. But such groups are also very central to the person-centred approach, on the basis that such structurelessness allows everybody to have space to speak: to create equality. But what she argues is that, if you have unstructured groups, what comes to the fore is the pre-existing power structures. Elites, those in power, recreate those power structures in a vacuum, and therefore you may need more active facilitation: people to hold open a space for everyone. You need, maybe, structures. You need leadership as a way of allowing and supporting equality to emerge.
So while the strength of the person-centred approach is that ability to really hear deeply the phenomenological experiencing, there is also something outside of that; the a priori, the before those structures that the person-centred approach, as it’s developed, as it’s practiced, may not fully take into account. And this raises challenges for the person-centred field. I think that’s why movements like Black Lives Matter, MeToo, have moved to a radical perspective. It’s moved away from, or moved on from, or moved apart from, what is a more traditional, classic, person-centred, humanistic understandings—towards one which emphasizes power and imbalance.
The counterpoint to that, though, is that if we move too far from a phenomenological understanding, that understanding of people in terms of intelligibility: if we just understand people in a structural sense, then we lose touch with the reality of people’s experiences. I know some people have argued that the backlash against ‘wokeism’ is because people feel that they’re being accused of racism or transphobia or other wrongs, and it just doesn’t sit with their conscious, phenomenological experiencing. Certainly, this is not to suggest that that is the only reason why there’s been a rise of the Far Right. But, perhaps, there is something about people feeling that they aren’t understood because it doesn’t match their phenomenological reality. So the challenge, and I think it’s a very important challenge, is, ‘How do we hold on to…? How do we combine…? How do we create synergies between a deeply phenomenological psychological equality that really values, respects, and understands that experiencing of the other as a human being like me; but can also recognize that that sits within structures—within powers that extend beyond the phenomenological experiencing?’ For Rogers, everything is subjective. And yet, if we collapse everything into the subjective, we lose that intersubjective, we lose that structure, we lose that relationality.
Evolving Synergies between Social Justice and the Person-Centred Approach
The challenge, then, is to find some kind of structured, embedded, contextualized phenomenology. To understand phenomenological experiencing and the actualizing tendency—that striving for maintenance and enhancement of self—but to understand that within structures: not just the conditions of worth, but also economic, social class, and cultural structures.
Actually, a lot of that is already there in the work of Karl Marx, and the parallels between Marx’s and Rogers’s writings are quite striking. This, for instance, is from Marx’s Kapital:
All means for the development of production transform themselves into means of domination over, and exploitation of, the producers; they mutilate the laborer into a fragment of a man, degrade him to the level of an appendage of a machine, destroy every remnant of charm in his work and turn it into a hated toil; they estrange from him the intellectual potentialities of the labor process in the same proportion as science is incorporated in it as an independent power, they distort the conditions under which he works, subject him during the labor process to a despotism the more hateful for its meanness; they transform his life-time into workingtime, and drag his wife and child beneath the wheels of the Juggernaut of capital.
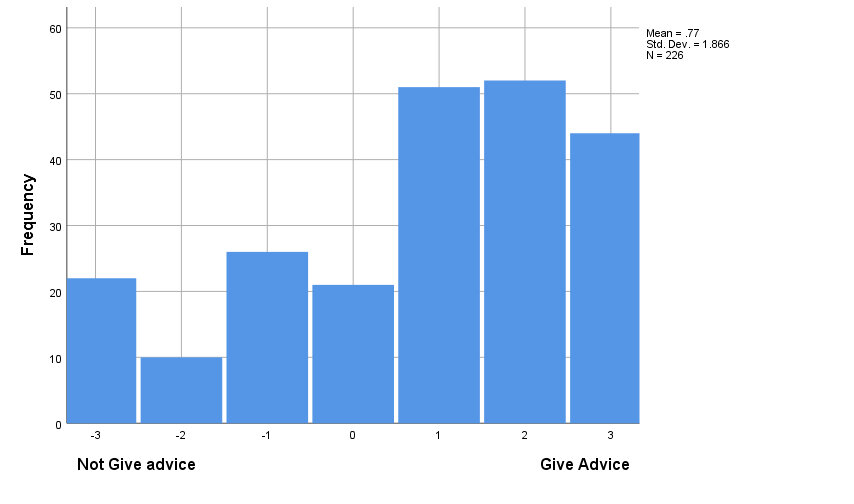
Here, we see that Marx combines that deep phenomenological understanding of self-estrangement—a distortion of the experiencing self, which Rogers also focuses on—but rather than understanding it wholly in psychological terms, Marx shows how our social and economic conditions can impact and inform our phenomenological reality. It’s something that I talk about in Psychology at the Heart of Social Change: the resources that we’re limited by and how they create internal conflict. What I argue is that, as we have more and more constricted resources then, psychologically, phenomenologically, what that does is to creates more internal conflict. It’s a bit like in chemistry: if you have a balloon and you squeeze it more tightly, the atoms bounce up more and more against each other. From a Rogerian standpoint, we are actualizing beings, meaning that we are always striving to maintain and enhance ourselves. But sometimes that can take us in different directions. There’s different things that we want to maintain and enhance. And as our resources become more and more limited, so we’re more and more forced to fight against ourselves. Rogers’s conflict between the desire for positive regard and the desire to actualise other wants and needs (like our sexuality or our sense of identity) is one example of that. In conditions where there’s very strict, conditional, positive regard, then we have to make choices about, ‘Do we actualise this or do we actualise that?’ And similarly, if we have limited economic resources—somebody who’s in a very impoverished environment—it’s not that they’re not actualizing. It’s not that they’re not still striving to maintain and enhance themselves, but they are forced more to fight against themselves and make more and more difficult choices, because to have A means that they can’t have B and vice versa. If we had unlimited resources, we could have A and B and C and D and everything that we wanted to, but as those resources become more limited, so the internal conflicts become more and more and more.
So that’s one way to develop a contextualised phenomenology, and I think that can also help us understand something of why is it that people can behave and think in ways that can really do a lot of harm and damage to other people, like the Far Right. We can understand the actualizing tendencies as operating always within a context, within a particular horizon. So rather than seeing, as Rogers tends to, that everything ultimately is aligned to a single formative tendency—that everything is ultimately for a greater good—we can understand people as acting in relation to their particular circumstances. For instance, somebody who’s driving a car to work when they don’t need to—that’s causing damage to the to the planet. We can’t say, ‘That’s not an expression of the actualising tendency’, because then we get into contradictions around the idea that sometimes people are driven by something other than actualisation (which Rogers describes as the one and only driving force). But what we can say is that, where somebody’s limited—and again, the more limited the resources, the more limited the horizon—the less far they can see: they can’t see the bigger picture, the full effect. In other words, the more limited the horizons, the more somebody might just look at their local context and just think, ‘Well, I’ve got to get to work. It’s really important to get to work. I’m stressed.’ So it is actualising. It’s a person striving to do their best in that circumstance, but because the resources are so limited, they can only see the very local context.
One of the things I talk about in a couple of recent books is the idea of rogue goals, and rogue goals is the notion that we can get caught up in local, immediate goals and miss the bigger picture. It’s not that we’re not actualizing. It’s not that we’re not directional. But we can get caught up in lower-level goals where we’re aiming for things that might seem or might feel that they’re maintaining or enhancing within that context, within the horizons that we can see. But within a broader horizon, within a broader context, they’re not actually the best thing for ourselves or for others. A classic example might be, for instance, using drugs. It’s not that someone who uses drugs isn’t trying to maintain and enhance themselves: they’re striving. It’s just that that drive is then opposed to other things that are healthy and things that they want, like good health. And we can think about that going all the way up: that people in a community or people in a class can become focused on just the goals for that class—just what that class wants—and lose sight of the bigger picture.
In terms of developing synergies, there’s also something about leadership. Sometimes, in the person-centred field, we can be very wary of leadership: we don’t want to tell people what to do. But I remember Pete Sanders always saying, ‘Don’t trust the process, organize the process’. Maybe if we recognise the risks of that actualizing tendency working towards local and lower-level kind of goals, rather than seeing the bigger picture, then we can see that there needs to be people who can be in those positions of leadership who can coordinate between different positions. Ideally, that is the role that a leader can play: not that they’re making the decisions, not that they have the power. But they’re able to coordinate between multiple perspectives and hold on to an idea of social justice and see that, when one person is striving for getting what they want… OK, that might be actualizing in that person’s context, but, actually, that could then damage others—the greater whole. What I’ve learnt in my time in the therapy field is that there’s such a desperate need for leadership, and particularly around social justice. In TaSC, we’ve had people coming in taking on leadership roles in such a supportive way to the community as a whole, and I think there’s a real ‘servant leadership’. I think it’s to the detriment of the person-centred approach if we don’t see ourselves as having the potential to take on leadership roles.
There’s also something about nuance: understanding that, if we combine structural perspectives with more phenomenological perspectives, things can get pretty complex. In the multicultural approach, they talk about the way that people can hold positions both of power and marginalization at the same time. That, for instance, as a white Jewish man, I have both privilege but also that I’m marginalized in certain ways. Some of the work around pluralism is trying to allow for heterogeneity, allowing for different perspectives. That is, allowing that tension, for instance, between class structures and community structures and psychological structures, and more messiness.
There’s also something very exciting to me about seeing parallels across different levels. If we use a concept like ‘configurations of self’—the idea that we will have different voices and parts within us—we can then think about the parallels between what goes on at an intrapersonal level, what goes on at an interpersonal level, what goes on between communities, and what goes on between nations. What are the kind of processes, for instance, that as a person-centred therapist we know work at the intrapersonal level: for instance, prizing different voices and engaging empathically. And we can think about how these processes—ways of maximising benefit—can operate across different levels. Similarly, thinking about democracy: that’s something we have a sense of is good within a nation. But then, what might it mean to have a democratic internal, psychological structure—between the configurations of self?
Finally, when thinking about social justice, I think it’s important to ask whether ‘person centred’ is the most helpful term? Will ‘person-centred’ always mean a focus on the individual and be in tension with a wider social justice perspective? And, for instance, how does that work with ‘transhumanists’ who think about animals and the environment. Do we need to think about other ways of articulating what we really believe in? In part, I guess this goes back to the question of the essence of a ‘person-centred’ approach? What is it really about? Is it a particular model of the person? Is it a particular ethic? Is it a particular set of values? Perhaps if we understand it as, most fundamentally, a set of values, then that might give it the greatest potential to align to a social justice perspective.
Conclusion
I hope I have conveyed, in this talk, my view that the person-centred approach has a unique contribution to social justice. It’s a trust in the intelligibility of the other: their deep, deep psychological equality. But I also think that the person-centred approach is not a complete theory of social justice—at least, not yet. And we have some choices, as a community, as a field, about whether we do develop the person-centred approach to be a practice fundamentally rooted in social justice, or whether we see social justice more as just a corollary of our clinical or ontological foundations. Personally, I would love to see the former, but it all comes down to how the person-centred approach is defined and conceptualised for the future. And, even as an approach that is defined primarily in clinical terms, it still has much to contribute to a fairer, more equitable society—one in which all citizens have an opportunity to thrive.
Acknowledgements
I am deeply grateful to the many people who have influenced and informed my work: John McLeod, Pete Sanders, Nicola Blunden, colleagues in the TaSC Network; and my partner Julie. Thanks to the organising group for the Melissa Harte lecture: Kurt Renders, Lou Cooper, Shari Geller, and Genevieve Rix. A very special thanks to John and Sandra Wilson at Onlinevents and their team, both for supporting this talk and also the very warm and kind support they have given to me, as a person, over the years.
Photo by Alexander Grey on Unsplash